Digital technologies is a profound contributor towards modern day healthcare and preventive medicine. A vast array of devices and software is now used across biomedical and health domains, with approximately 260,000 health and medical apps demonstrating the staggering level of accessibility (Lupton, 2017). Contemporary digital health has now positioned lay people as both active and passive consumers of health and medical information, thus intertwining lay and professional knowledge and expertise (Lupton, 2017). Patient self-care technologies, search engines, health care websites, Telemedicine and social media are some major examples of digital health which has paved the way towards contemporary health care.
A major critical aspect of digital health is removal of the traditional face-to-face care. When the physical aspect has been taken out of consultations, forms of “invisible labour” are required on behalf of the health care professionals. Additionally, the physical-examination by a doctor often inspires trust in the patient whilst portraying empathy and care (Lupton, 2017). Without this patients must seek other ways to determine the level of trust for their doctor. Furthermore patients may be required to perform their own physical-examinations, which raises concerns on the validity of the data. Patient self-care technologies have drastically assisted the “do-it-yourself” process fostering the ideology of empowered patients, however the fallibilities and limitations of these technologies are often not acknowledged by the provider (Lupton, 2017). Contemporary digital health now implicates that health professionals must ask different forms of questions that compensates for the lack of the personal interactions and deciphers the digital information provided.
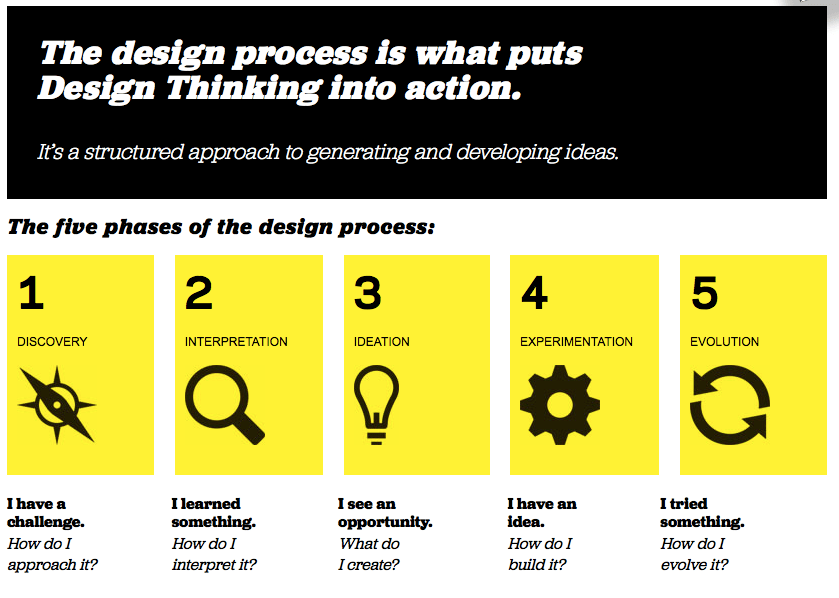
Design Based Thinking (DBT) is a creative process that helps design meaningful solutions in the classroom, the school and the community. The five phases of digital thinking (as above) demonstrates a pedagogical process that can be effectively utilised within digital health.
My Anecdotal experience with DBT
We were asked to randomly chose on element from the 4 categories; a body part/system, a demographic, a location, and a feeling. Our group selected had selected Blood, Children, the home and reassured. Then Using guided questions we were to collaboratively think of a related health problem and brainstorm a digital invention that would provide aid and could be used within the context we had randomly created. Then using the storyboard activity (pictured below) we envisioned a real world scenario where our invention could be practically used.


Reflecting on Bloom’s taxonomy and 21st century pedagogies in relation to DBT
Using these frameworks a talented teacher can scaffold the DBT activities to tailor the level of learning to the individual. Additionally an effective activity can incorporate all discipline areas for the 21stcentury learner. “In today’s world, it’s no longer how much you know that matters; it’s what you can do with what you know” (Wagner & Danchin, 2010, p. 111). Thus DBT is an effective way to encourage students to “use” their health knowledge to “create” change within the community. The above example shows that when DBT is done with a collaborative approach it reach all disciplines that umbellar under the engaged thinker, ethical citizen and entrepreneurial spirit.


Reference:
Lupton, D. (2017, April 16). Design Sociology part 1: a research agenda [Web blog post]. Retrieved from https://simplysociology.wordpress.com/2017/04/16/design-sociology-a-research-agenda/
Lupton, D. (2017, April 21). Design Sociology part 2: terms and approaches [Web blog post]. Retrieved from https://simplysociology.wordpress.com/2017/04/21/design-sociology-part-2-terms-and-approaches/
Wagner, R. H., & Danchin, É. (2010). A taxonomy of biological information. Oikos, 119(2), 203-209.
